Keeping Your Job When You Need Dialysis

If you are working when you learn your kidneys are failing, some of your most urgent questions may be about your job. Each year, half of all people who start dialysis in the U.S. are under 65. You are not alone. It is possible to feel well enough to work on dialysis and to make your treatment schedule fit your job—IF you plan ahead. We'll tell you why—and how—to keep your job.
Fight fatigue
Do you feel too tired to work? Failing kidneys make less of a key hormone, erythropoietin (EPO). EPO tells your bone marrow to make red blood cells, which bring oxygen to your cells. When you don't have enough red blood cells, you have anemia. Most people with stage 4 or 5 chronic kidney disease (CKD) have anemia, which can make you feel:
- Tired
- Weak
- Short of breath
- Mentally fuzzy
- Cold all the time
Anemia can also cause pale lips, gums, and nail beds. In men, it can cause erectile problems. And, some people crave ice, clay, laundry starch, or dirt when they have anemia.
Anemia can be treated, and you can have more energy. But many people don't get treatment. Sadly, some even quit their jobs, thinking they'll never feel well enough to work. By the time they start dialysis and get their anemia treated, it's often too late to go back.
Don't let this happen to you! Anemia can come on slowly. You may not notice it at first. Ask for a blood test to be sure. If your red blood cell level is low, talk with your doctor. Iron pills and a form of EPO called Aranesp® or Procrit® are used to treat anemia. NOTE: The FDA has put a "Black Box" warning on EPO drugs, which have caused harm in some people with cancer or heart problems. Talk with your doctor about the risks and benefits for YOU—and keeping your job.
Earn more than disability pays
Permanent vacation...no deadlines, no more boss. Sound good? What most people don't know is that Social Security Disability Insurance (SSDI) may only pay about 35% of what you earn at work. To prevent fraud, even a private disability plan will replace just 60% of work income (minus SSDI payments). 1 This means most people can earn much more money from work than they would get from disability.
Think about it: what would you have to do without if you had just 1/3 or even 2/3 of your current income? Could you keep your home? Your car? Could you eat a meal out or take a trip? Could you help send your kids to college?
Think long and hard before you decide to take disability. Once you do, it can be very hard to go back to work in the future.
Stay healthier and feel better
Research shows that people on dialysis who keep their jobs feel better. They are more physically able, with less pain. They have better general health and energy. 2 And better physical function means they may have fewer and shorter hospital stays—and live longer. 3 Of course, people who feel better in the first place are more likely to work. But a job can also give you a sense of purpose, a place to be, an identity, and income. Those things can help you feel good about yourself and your life.
People with CKD who work are also far more likely to have a health plan through work. 4 An employer group health plan (EGHP) can help pay for treatment and drugs Medicare does not cover. You may be better able to afford to follow your care plan if you keep your job.
Choose a work-friendly option
Plan ahead if you can. You know your work schedule and whether your job includes travel. If you have a living donor, you may be able to plan to get a kidney transplant before you need dialysis. This is preemptive transplant. If not, choose a form of dialysis that will be "work-friendly" so you can:
- Work during normal work hours
- Travel for work if you need
- Feel your best between treatments
- Have a normal or near-normal diet
Standard in-center hemodialysis

Dialysis clinics offer hemodialysis (HD) three times a week (MWF or TRS). A plastic filter called a dialyzer cleans the blood. Blood goes to the dialyzer through tubing that connects to two needles in your arm. Treatments last 3–4 hours (just 9–12 hours out of 168 in a week), so they require strict diet and fluid limits, and you need to take (and pay for) many meds.
You may be able to get a shift early in the morning or in the evening after work. For some, this is work-friendly. They bring a laptop and/or cell phone (if the clinic allows it) and do work. For others, the "dialysis hangover" of taking off extra fluid just three times a week leaves them washed out, with flu-like symptoms after treatments, and fuzzy thinking all the time.
In-center nocturnal HD
What if you could get treatments at night, while you sleep—in the clinic? This is in-center nocturnal HD, and more clinics are starting to offer it. These treatments don't take time out of your work day. With more than twice as much treatment, people feel better, stay out of the hospital more—and live longer. 5 Plus, there are fewer meds to take and fewer fluid limits. Treatments tend to start at 8 or 9 pm and end at 4 or 5 am.
Peritoneal dialysis
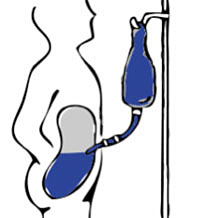 PD uses the inner lining of the belly (the
peritoneum)
as a sac to hold sterile fluid. Fluid goes in through a plastic tube (catheter) placed by a surgeon. Wastes and excess water flow into the fluid. Used fluid is drained out and fresh is put in, in a process called an
exchange.
No needles are used for PD, and your blood stays in your body. Since your blood is cleaned most or all of the time with PD, there is no "dialysis hangover" and your meal plan will be more normal. You can do:
PD uses the inner lining of the belly (the
peritoneum)
as a sac to hold sterile fluid. Fluid goes in through a plastic tube (catheter) placed by a surgeon. Wastes and excess water flow into the fluid. Used fluid is drained out and fresh is put in, in a process called an
exchange.
No needles are used for PD, and your blood stays in your body. Since your blood is cleaned most or all of the time with PD, there is no "dialysis hangover" and your meal plan will be more normal. You can do:
- Continuous ambulatory PD (CAPD)
- Do exchanges by hand at breakfast, lunch, dinner, and bedtime. Bring a bag to work to do a lunchtime exchange (you'll need a clean room to avoid infection).
- Continuous cycling PD (CCPD)
- Use a cycler machine to do exchanges at night while you sleep. You may also need to do one daytime exchange by hand.
Home HD

If you choose home HD, you can do your treatments on your own time—like morning one day and evening the next. Your clinic will provide a machine, supplies, and training. (You don't have to buy a machine.) Most programs will want you to have a partner to train with you and be there in case you need a hand. Home HD is very work friendly:
- Nocturnal home HD (NHHD)
- Do treatments at night while you sleep, 3–6 nights per week. NHHD leaves your days free for work, and offers a normal or near-normal diet and fluids, with fewer drugs and no "dialysis hangover."
- Daily home HD (DHHD)
- Do short (2–3 hour) treatments 5–6 days a week in the early morning or after dinner while you watch TV. The frequent treatments prevent "dialysis hangover," and the diet is more normal than in-center HD.
- Conventional home HD
- Do treatments three times a week (or every other day) on your own schedule at home. Dialyze longer if you need to remove more fluid and wastes.
Find a center that offers your choice
Many of the 5,200 or so dialysis centers in the U.S. offer in-center HD only. You may have to do some homework to find a center that offers a more work-friendly option. About 40% of U.S. centers have PD, and about one in ten has home HD.
You may also need to change doctors if your doctor does not support your choice. Research shows that people who choose their dialysis option themselves live longer. And, they are more likely to get a transplant than those whose doctor chooses for them—or even those who work with their care teams to make a choice. 6 This makes sense, since you're the one who must live with your choice each day.
On the Home Dialysis Central website, there is a database of U.S. clinics that offer home or in-center nocturnal treatments.
You can look up clinics by state, or even by your town. If you live near a state border, the nearest center may be in the next state.
Once you find a center, you will see contact information, which treatments it offers, and a map to help you find it.
Plan for your training and set-up needs
It takes a week or two to train for PD. Most programs will do a home visit to help you choose a room for PD exchanges and figure out where you will store your supplies.
You may be able to use vacation or sick days to have your PD catheter placed and train for PD. If you know this is coming, you can plan to save up your vacation or sick days. Or, if your company is large enough (50 or more employees), you may be able to use the Family and Medical Leave Act (FMLA) to ask for unpaid time off. Plan on one clinic visit per month to check your blood pressure, do blood tests, review your treatment logs, and see if you need any changes to your treatments. If you get an infection, you may miss some work time.
Training for home HD takes longer—usually 3–6 weeks. Many programs require a home visit. For some older types of machines, plumbing and wiring changes are needed to your home. Some centers will pay for this. Others will pass these costs on to you.
You may need to take a temporary leave of absence from work for your access surgery and home HD training, unless you have enough vacation or sick time. Your home HD partner will also need to take some time off work, since training is mostly done during work hours. Talk with the home training nurse if this is a problem. You may be able to arrange a training schedule that will minimize time lost from work.
Conclusion
Kidney failure will change your life—but how much and in what ways is largely up to you. Plan ahead and choose a work-friendly treatment to feel your best and reduce the impact of CKD on your lifestyle and income. To learn more, download and read A Kidney Patient's Guide to Working and Paying for Treatment .
References:
- Insurance Information Institute website, accessed June 25, 2010.
- Blake C, Codd MB, Cassidy A, O'Meara YM. Physical function, employment and quality of life in end-stage renal disease. J Nephrol; 13(2):142-9, 2000.
- Lowrie EG, Curtin RB, LePain N, Schatell D. Medical outcomes study short form-36: a consistent and powerful predictor of morbidity and mortality in dialysis patients. Am J Kidney Dis. 2003 Jun;41(6):1286-92.
- USRDS special data request, May 20, 2003. The data reported here were supplied by the United States Renal Data System (USRDS). The interpretation and reporting of these data are the responsibility of the author(s) and in no way should be seen as an official policy or interpretation of the U.S. government.
- Lacson E Jr, Wang W, Lester K, Ofsthun N, Lazarus JM, Hakim RM. Outcomes associated with in-center nocturnal hemodialysis from a large multicenter program. Clin J Am Soc Nephrol. 2010 Feb;5(2):220-6.
- Stack AG, Martin DR. Association of patient autonomy with increased transplantation and survival among new dialysis patients in the United States. Am J Kidney Dis 45(4):730-742, 2005.